The Evolution of Health Care Reform
The ACA uses Medicaid to get health insurance to millions of people. Colleen Grogan is keeping track of what happened after that plan was derailed.
By Carl Vogel
VOLUME 21 | ISSUE 2 | SUMMER 2014
The timing couldn't have been much better. Three months after the landmark Affordable Care Act passed in 2010, SSA Professor Colleen Grogan became editor of the Journal of Health Politics, Policy and Law.

ABSTRACT
SSA Professor Colleen Grogan has written extensively on the political evolution and current politics of the Medicaid program and the historic development of public health care spending through private entities in the U.S. health care system. When the Affordable Care Act was passed, it was written to add as many as 16 million low-income people to Medicaid, but Supreme Court ruled that the federal government couldn’t require states to adopt the expansion. Nearly half the states have not expanded the program, leaving approximately 5 million very low-income individuals without health care insurance. Grogan has been studying the dynamics of which states have and have not expanded Medicaid under the ACA, including the historical, racial, demographic and political factors that are having an impact.
________________________________________________________________________________________________________
For Grogan and other leading scholars in health care policy, the ACA has been a once-in-a-generation opportunity to explore the political, legal and programmatic dynamics of health care reform in the United States. Created to fit into America’s fractured health care system and forged through a contentious political process, the law is a complex mixture of public and private insurance systems with a mix of roles for federal and state policy makers.
Grogan has been watching with a keen eye from the start. The academic director of SSA’s Graduate Program in Health Administration and Policy (GPHAP) and the co-director of SSA’s Center for Health Administration Studies (CHAS), she has written extensively on the political evolution and current politics of the Medicaid program and the historic development of public health care spending through private entities in the U.S. health care system.
Much of the attention in the mainstream press has been focused on the rollout of the federal website and how many Americans signed up for the new health insurance exchanges. But to reach its goals, the ACA was written to expand Medicaid coverage to a wider population, aiming to add as many as 16 million low-income people to the program, roughly half the total expected to gain health care insurance through the ACA.
From when it was first passed and through a number of expansions over the years, there have always been gaps in who is covered by Medicaid. “The ACA brings in millions of new people by adding single males, childless couples and the homeless, whose incomes are below 138 percent of the federal poverty level [about $16,000 a year for a single adult],” Grogan says. “It also adds anyone whose income is below that level but currently above the threshold their state has set.”
Those plans changed dramatically, however, when the Supreme Court ruled that the ACA individual mandate was constitutional—but that the federal government couldn’t require states to adopt the Medicaid expansion. Suddenly, a key section of the ACA’s quilt of coverage was no longer guaranteed.
Thanks to a quirk in how the law was written, if a state decides not to expand Medicaid, people between 100 percent and 138 percent of the poverty level are eligible to receive financial help on the insurance exchanges. But there’s a gap in coverage for adults whose income is below 100 percent of the poverty level but still too high for their state’s current Medicaid rules.
To date, although 27 states (including the District of Columbia), have agreed to expand Medicaid, the rest have not. The current estimate is that about 5 million low-income individuals will fall into the coverage gap between what was planned for Medicaid expansion and today’s reality.
“Medicaid expansion is the most important public health aspect of the ACA, and it is shoring up the safety net in the states that have embraced it,” says Harold Pollack, SSA’s Helen Ross Professor and an executive committee member at CHAS. “Colleen’s work has explored the impacts of Medicaid expansion and the mixture of factors and forces that are keeping that from happening in many states.”
Although the fallout from the option to refuse to expand Medicaid may be the biggest unexpected turn of events in the rollout of the ACA, it is far from the only one. Grogan’s wide-ranging expertise on the forces that have built our current health care system give her a unique perspective on these unintended consequences and complicated outcomes. For an expert on how Medicaid impacts the lives of Americans living in poverty like Grogan, it’s an unbelievably busy time.

Click here to view the full-sized maps
{kind=link}
When Grogan talks about the future of Medicaid, she usually starts by pointing out some common misunderstandings about its past and its present.
Even before the ACA, Medicaid was the country’s largest health insurer, public or private, with 58 million enrollees in 2008, or one in five Americans. Partly that’s because Medicaid is much more than health care for the very poor. The program pays for the long-term care for 70 percent of all Americans in nursing homes, for instance, 44 percent of the health services to AIDS patients, and the premiums and drug costs of 20 percent of Medicare patients.
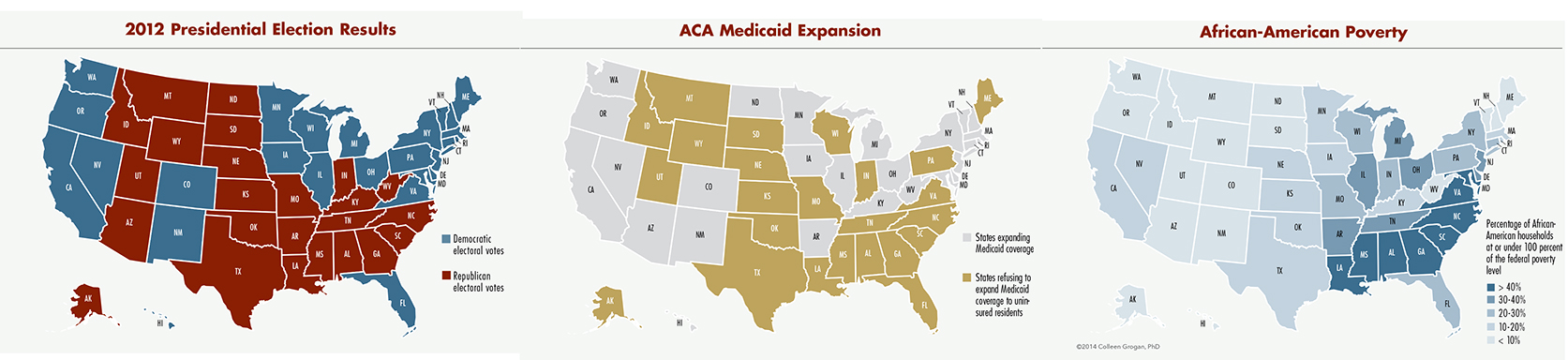
At first glance, it might simply look like blue states have expanded Medicaid under the ACA while red states have not, but there’s more to the story. For example, Republican governors in Arizona, Michigan, North Dakota and Ohio—all of whom signed on to the lawsuit against the ACA—have persuaded bipartisan legislatures to adopt the Medicaid expansion. The reason, Grogan says, is basically due to the same two compelling forces that have pushed states to participate in Medicaid’s growth over the last 40 plus years: Intergovernmental financing has created a strong inducement for states to expand Medicaid to leverage federal dollars, and the majority of citizens have favored using the program to expand health coverage.
With the ACA, the federal government is required to pay 100 percent of the costs of Medicaid expansion through 2016 and never less than 90 percent thereafter. And in a study examining what factors influence state decisions around the Medicaid expansion, Grogan and SSA doctoral student, Sunggeun Park, find that most states actions are congruent with what polls say is the majority will in the state.
However, Grogan and Park have also found that race also plays a role, notably that states with a higher proportion of the population that is African-American are less likely to adopt the Medicaid expansion. This relationship is due in part to differences in public opinion by race. While 45 percent of whites support expansion, 82 percent of African-Americans support it and 64 percent of Latinos and others support it.
Grogan and Parks have found that when it comes to Medicaid expansion, states are less responsive to minority public opinion. They used a relatively new political science model that measures the tipping point of the level of public support required for a policy or program before a state will adopt it. The politically “safer” and less controversial an issue is, the less public support is necessary for it to become law.
For Medicaid expansion through the ACA, when looking only at the white population, states tend to adopt the Medicaid expansion at a threshold of public support of 45 percent. However, when estimating state adoption with Latinos and African-Americans also added to the model, Grogan and Parks found that the average public support needed increases to 55 percent. “The public support of Latinos and African-Americans for expansion doesn’t appear to register with lawmakers as much as white support,” Grogan says. “If it did, the tipping point wouldn’t move so dramatically when those groups are out of the equation.”
The consequences of this gap are stark. The majority of the 5 million people who would benefit from the ACA Medicaid expansion where it is not being adopted are in the South, in large part because these states have high poverty rates and very restrictive current Medicaid eligibility levels. Grogan also notes that in most Southern non-expansion states—Maryland, Virginia, North Carolina, South Carolina, Georgia, Alabama, Mississippi and Louisiana—more than 40 percent of black households have incomes below the federal poverty level.
“This raises questions about the protection of minority rights and whether the denial of access to public health insurance benefits in states that rejected the Medicaid expansion is fair and just,” Grogan says.
“We’re in a situation now where the low- and middle-income households are getting more subsidies because the exchanges are open, and high-income individuals continue to get employer based tax-exemptions, but millions of very poor people—including many people of color—still have no coverage because they live in states that haven’t opted to expand Medicaid,” she says. “It’s hugely regressive, and considering the history of racial exclusion for social justice programs like the New Deal, it’s a real injustice. It’s the biggest problem with the ACA and the majority of Americans have no idea what’s going on.”
Despite the current situation, Grogan predicts that all 50 states will eventually adopt the Medicaid expansion. Partly that’s simply the ebb and flow of politics. “When Obama goes out of office—certainly if a Republican comes in—then they can say, ‘Now we can work with the federal government,’” she says. “And even if a Democrat wins, that can be enough to have it be a ‘new direction.’”
Why would deeply conservative states be willing to make the move? Grogan points again to the two factors that have historically helped convince states to sign on as Medicaid grows.
The first is federal funding, which is important to a constituency that is more powerful than low-income patients: hospitals and medical groups. The Urban Institute and Robert Wood Johnson Foundation estimate that if all states expanded Medicaid, hospitals would earn $293.9 billion in additional revenue from 2013 to 2022. Turning down Medicaid expansion means turning down the state’s portion of those federal funds.
Making the situation worse, a provision was written into the ACA that reduces existing federal funding that goes to hospitals when they provide services for patients without insurance. When the ACA was passed, the logic was that poor uninsured citizens would be covered by Medicaid across the country and thus there would be no need to reimburse hospitals beyond the ACA insurance subsidies. Of course, for hospitals in states that haven’t expanded Medicaid, that now means both forgoing access to new Medicaid funding and losing an existing income stream.
“All public hospitals in the U.S. are desperate for sufficient funding,” Pollack says. “And now the large public hospital systems in states like Florida and Georgia are facing real financial trouble. These are interest groups that are going to be calling for states to take this money. In a lot of places, that’s already happening.”
The other historic factor is how public opinion can grow. Much of what Medicaid currently covers are services like long-term health care for the elderly and help to people who are disabled, which serve many households that are far above the federal poverty line. Grogan emphasizes that the majority of these state Medicaid expenditures are optional—something the states chose to do on their own without federal requirements. Indeed, only six states spend less than half of their Medicaid dollars on optional services.
“Groups like nursing homes and the elderly population put pressure on states to say we want this option,” says Grogan, who argues that a powerful force in Medicaid’s history is that as it keeps expanding, it builds its constituency of supporters. Her research has found, for example, that adults whose parents received Medicaid benefits are more likely to oppose spending cuts to the program, with support rising from 52 percent to 64 percent.
This growth in support is part of the reason why conservatives are so resistant to the ACA expansion of Medicaid. Grogan has estimated that full expansion by 2019 would cover more than a quarter of the total population in 15 states, including Tennessee, Alabama and South Carolina, and more than a third of the residents in six states, including Louisiana and Mississippi.
“States know that it will be very difficult to turn back the clock when over 30 percent of your state’s population is covered by Medicaid,” she says. “Based on what we’ve seen with other groups, people fight much harder to keep a benefit once they’ve had it in their lives.”
The distinction and interaction between the public and private health care systems—and how politicians often blur the lines to make policies and programs more palatable to voters—has been a major research topic in Grogan’s work and is the subject of her next book. In many ways, she says, the American public is unaware of how much of what we consider private health care is connected to public funding.
With the ACA’s federal regulation of private insurance markets, mandatory purchase of private insurance, and government-created exchanges where many families will have part of their private insurance paid for with federal dollars, health care reform provides Grogan with a wealth of material. In Arkansas, Medicaid expansion provides another case study.
Last year, Arkansas’ Democratic governor Mike Beebe worked with the Republican-controlled legislature to hammer out a new approach. Starting in 2014, Arkansas is accepting the federal dollars available to the state to expand Medicaid. Rather than have those eligible enroll into the program, however, the state will allow them to shop for private insurance on the health care exchanges, like any other household, and then pay for their premiums with ACA Medicaid dollars.
“It’s an interesting approach and another example of hiding the role of public funding through private provision,” Grogan says of what’s being called the premium plan. “If Arkansas had just taken up expansion, something like 30 or 35 percent of the state’s population would be on Medicaid, and the legislators just couldn’t stomach that. With this, they can talk about it as private insurance, but it still means that some of the poorest people in the state get publicly funded health care coverage.”
Grogan also points out a twist to the story: “The [insurance companies] won’t know if the person they’re working with is on Medicaid or not. That’s actually pretty revolutionary, because poor people have never had access to the same providers as everyone else. Research shows that providers act differently when someone comes in and pays with Medicaid, and many providers don’t take Medicaid patients at all.”
Iowa has adopted a version of the premium plan, and the idea is being considered in Pennsylvania as well. The option is still controversial for some conservatives, though. The Nebraska legislature rejected a premium plan in the spring, and Republicans in the Arkansas legislature went through a bruising battle earlier this year about whether to continue with the program, which the Associated Press described as a “stalemate [that]... threatens to turn Little Rock into a small-scale version of the Washington budget battle that shut down the federal government for 16 days last year.”
Since taking the reins as editor of the Journal of Health Politics, Policy and Law, Grogan has expanded its editorial reach to help scholars share their research, thoughts and expertise on these kind of topics. “For the first issue, we did ‘Critical Essays on Health Care Reform’ and got some of the best people in the country on these issues,” she says. “We also had an issue titled ‘Affordable for Whom?’ which considered the adequacy of the ACA subsidies for low-income Americans, and whether the distribution of subsidies is fair across all income levels.”
Grogan has also started many special sections in the journal, the most recent of which is “The Implementation of Health Care Reform.” Recognizing the lag time between when an academic research project is ready for publication and the relative immediacy of how the ACA is unfolding, Grogan started the new section to allow researchers to publish their thoughts and observations on a topic.
Funded by the Robert Wood Johnson Foundation, “the essays are open access so that the work can be widely disseminated not only to academics but policymakers across the 50 states,” she says. “Because it is not part of the regular peer review process, we can be more responsive to topics happening now on the ground. I’m proud of the fact that we have both peer-reviewed research that can hold the test of time and shorter, timely essays to respond to issues states are currently grappling with.”
Grogan is also the project director for a new website, ACA Scholar-Practitioner Network. ASPN acts as a central portal for research on the implementation of the ACA at the state level. Hosted by SSA, the website has tabs organized by states, authors and topic, providing a one-stop source for information on the ACA, from cost-share limitations on the exchanges to Medicaid’s preventive health services.
“For scholars, this can be a way to increase collaboration—to find out who else is working on an issue you’re interested in—and a precursor to a literature review,” says the website’s coordinator, Phillip Singer, a doctoral student at the University of Michigan’s School of Public Health. “We also see it as a way to integrate various stakeholders involved with the ACA: policymakers, researchers, practitioners.”
“There can be such a disconnect between policymakers in the throes of trying to implement this complicated new law and the academics who are studying it,” Grogan says. “The ACA is clearly changing health care for low-income individuals in many, many ways—we want to figure out what’s working, how states can improve on implementing this complex program and how the states can be more democratically responsive to their citizens’ desires.”